When your body reacts to something harmless-like pollen, a food, or even heat-it’s not always an allergy in the classic sense. Sometimes, it’s your mast cells going haywire. These tiny immune cells sit at the front lines of your skin, lungs, and gut, waiting to respond. But when they activate too easily or too often, they dump out a storm of chemicals that cause hives, stomach pain, brain fog, flushing, and even anaphylaxis. This isn’t just allergy-it’s Mast Cell Activation Syndrome (MCAS), a real and growing condition affecting an estimated 1 in 1,000 to 1 in 10,000 people.
What Happens When Mast Cells Activate?
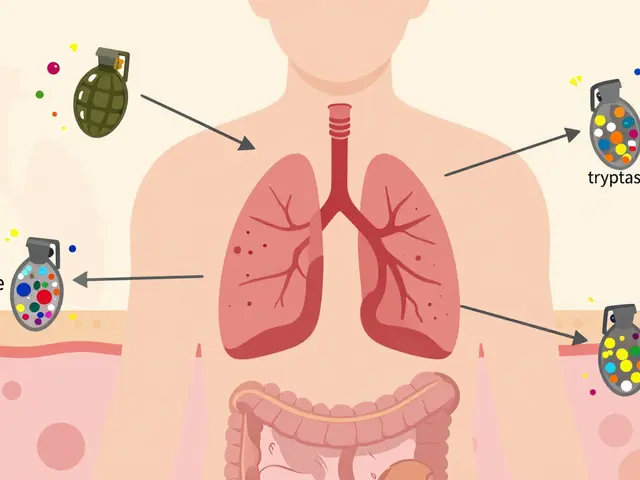
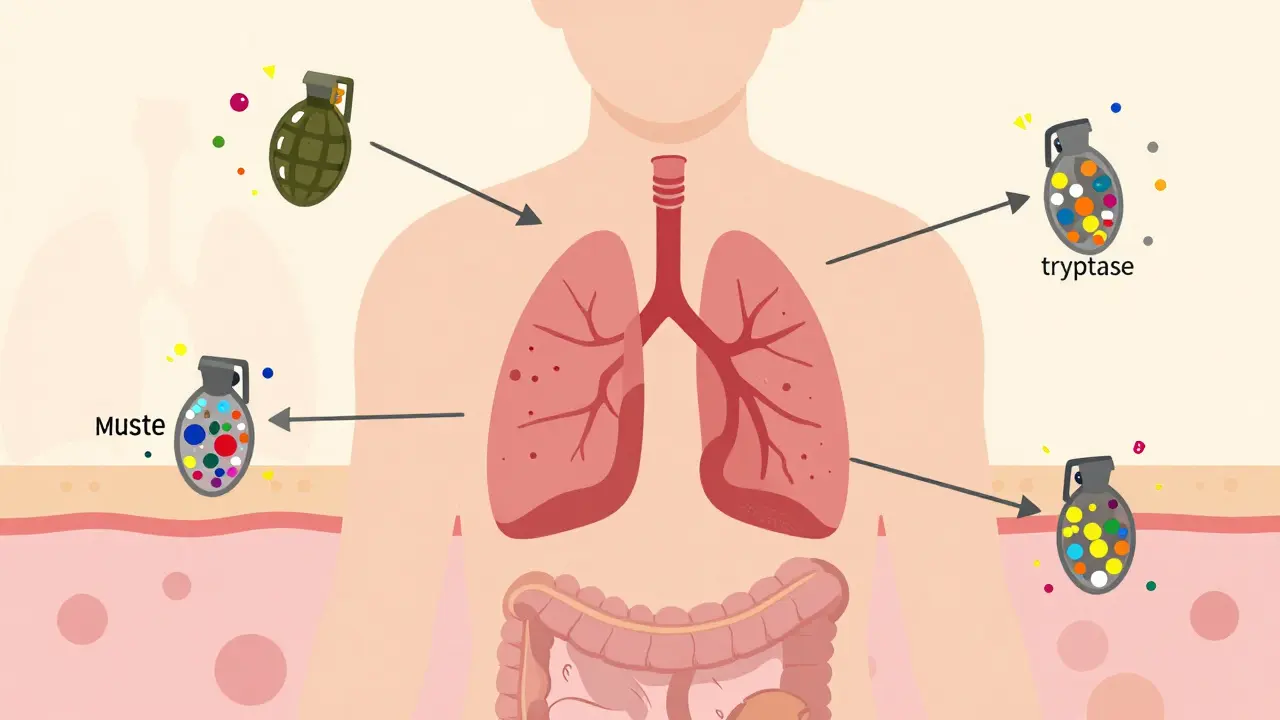
Mast cells are like loaded grenades. They sit quietly until triggered, then explode with chemicals stored inside them. These chemicals aren’t random-they’re carefully organized and released in stages. The first wave comes within seconds: histamine, tryptase, and chymase burst out of granules. Histamine alone makes up 10-15% of the granule’s dry weight. That’s why people with MCAS get sudden itching, swelling, or a runny nose within minutes of exposure.Then, within minutes, new chemicals are made on the spot: prostaglandin D2 (PGD2), leukotriene C4 (LTC4), and platelet-activating factor (PAF). These cause longer-lasting inflammation, congestion, and smooth muscle tightening-think asthma flare-ups or cramping intestines.
Hours later, the cytokine wave hits: IL-6, TNF-α, IL-13. These are the signals that turn up the immune system’s volume across the whole body. That’s why MCAS patients report fatigue, joint pain, and brain fog that lasts for days.
What triggers this? It’s not just IgE antibodies (the classic allergy pathway). About 70% of allergic reactions use IgE, but mast cells respond to dozens of other signals: stress, heat, NSAIDs like ibuprofen, alcohol, certain foods, even physical pressure or emotional trauma. A 2022 survey of over 1,200 MCAS patients found 68% react to NSAIDs, 63% to alcohol, and 57% to heat. These triggers don’t show up on standard allergy tests, which is why so many people are misdiagnosed for years.
How Mast Cell Stabilizers Work
Most allergy treatments focus on blocking the chemicals after they’re released-antihistamines block histamine, leukotriene inhibitors block LTC4. But mast cell stabilizers do something different: they stop the explosion before it happens.The most well-known stabilizer is cromolyn sodium, approved by the FDA in 1973. It works by preventing calcium from flooding into mast cells. Calcium is the signal that tells the cell, “Release everything now.” No calcium influx? No degranulation. That’s why cromolyn isn’t a rescue drug-it’s a preventive one. You have to take it before exposure, not after symptoms start.
Another option is ketotifen, approved in the U.S. in 1990. It does double duty: it stabilizes mast cells and also blocks histamine receptors. Studies show it reduces MCAS symptoms in 50-70% of users at doses of 1-4 mg twice daily. But it’s not perfect. Neither drug stops cytokine production. That’s why some patients still feel tired, achy, or mentally foggy even when their hives are gone.
Think of it this way: antihistamines are like putting out fires. Stabilizers are like locking the matches away. You can’t stop every fire, but you can stop a lot of them from starting.
Who Benefits Most From Stabilizers?
Not everyone with MCAS responds. A 2022 survey found 87% of patients saw *some* improvement with stabilizers, but only 43% got full control. That’s because MCAS isn’t one disease-it’s a spectrum. Some people have mostly histamine-driven symptoms. Others have cytokine overload. Stabilizers help best when the problem is degranulation.Patients with food-triggered flushing, chronic hives, or post-meal nausea often respond well. Those with severe brain fog or long-term fatigue may need more. Some people need combination therapy: stabilizers plus low-dose antihistamines, plus dietary changes.
One case documented on MastAttack.org involved a 42-year-old woman who had 70% fewer anaphylactic episodes after starting cromolyn at 200 mg four times a day. But it took 8 weeks. That’s the catch: stabilizers are slow. They don’t work like epinephrine. You have to stick with them.
The Real Challenges of Treatment
The biggest problem? Getting diagnosed. On average, MCAS patients see 6-10 doctors over 3-5 years before getting the right label. Many are told they have anxiety, IBS, or chronic fatigue syndrome. That’s because the symptoms are messy: headaches, diarrhea, dizziness, heart palpitations, rashes-all of which can look like other conditions.Even when diagnosed, treatment isn’t straightforward. Cromolyn sodium comes as a bitter liquid. A 2019 patient survey rated its taste 2.1 out of 5. Nearly 1 in 5 pediatric cases require feeding tubes just to get the dose in. And 35% of users report nausea or diarrhea-enough that 15% quit.
Testing for MCAS isn’t easy either. Doctors check serum tryptase (normal is under 11.4 ng/mL), but a spike only happens in about 30% of cases. More reliable markers are 24-hour urine tests for methylhistamine (normal under 1.3 mg) and N-methyl-β-hexosaminidase (normal under 1,000 ng/mg creatinine). A successful response means a 30% drop in these numbers.
And then there’s the trigger wheel. The community-created Mast Cell Trigger Wheel (from TMSforaCure.org) lists over 50 common triggers. Eliminating them all? Nearly impossible. Most people focus on the top 5: NSAIDs, alcohol, heat, stress, and certain foods. Even small exposures can set off a cascade.

What’s Next? Beyond Stabilizers
Mast cell stabilizers are helpful, but they’re not the whole story. In 2023, the FDA approved avapritinib for advanced systemic mastocytosis, a drug that targets the KIT D816V mutation found in 30% of MCAS patients. It’s not for everyone-but it’s a sign of where things are heading.Researchers are now testing drugs that block SYK kinase, a key signal in mast cell activation. In Phase II trials, 100 mg daily reduced mediator release by 75%. KIT inhibitors, mast cell-specific monoclonal antibodies, and combination therapies are all in development. By 2030, experts predict these next-gen drugs could control symptoms in 80-90% of patients.
For now, stabilizers remain the most accessible tool. They’re not glamorous. They don’t give instant relief. But for many, they’re the difference between constant flares and a life that’s manageable.
Practical Tips for Starting Stabilizer Therapy
If you’re considering mast cell stabilizers:- Start low: Cromolyn usually begins at 100 mg four times daily, taken 15-30 minutes before meals and bedtime.
- Go slow: Increase by 100 mg every 1-2 weeks if tolerated. Most people need 200-400 mg four times daily.
- Be patient: It can take 6-12 weeks to see real changes.
- Track symptoms: Use a daily log of triggers, symptoms, and medication timing.
- Test: Ask your doctor for urine methylhistamine and N-methyl-β-hexosaminidase tests before and after 3 months.
- Support: Join patient communities like the Mast Cell Disease Society-they have verified specialist directories and practical guides.
Stabilizers won’t fix everything. But for many, they’re the first real step toward regaining control.